
Multiple layers for safety: public health is not an à la carte menu.
Successful safety interventions are about a comprehensive commitment to the common good.
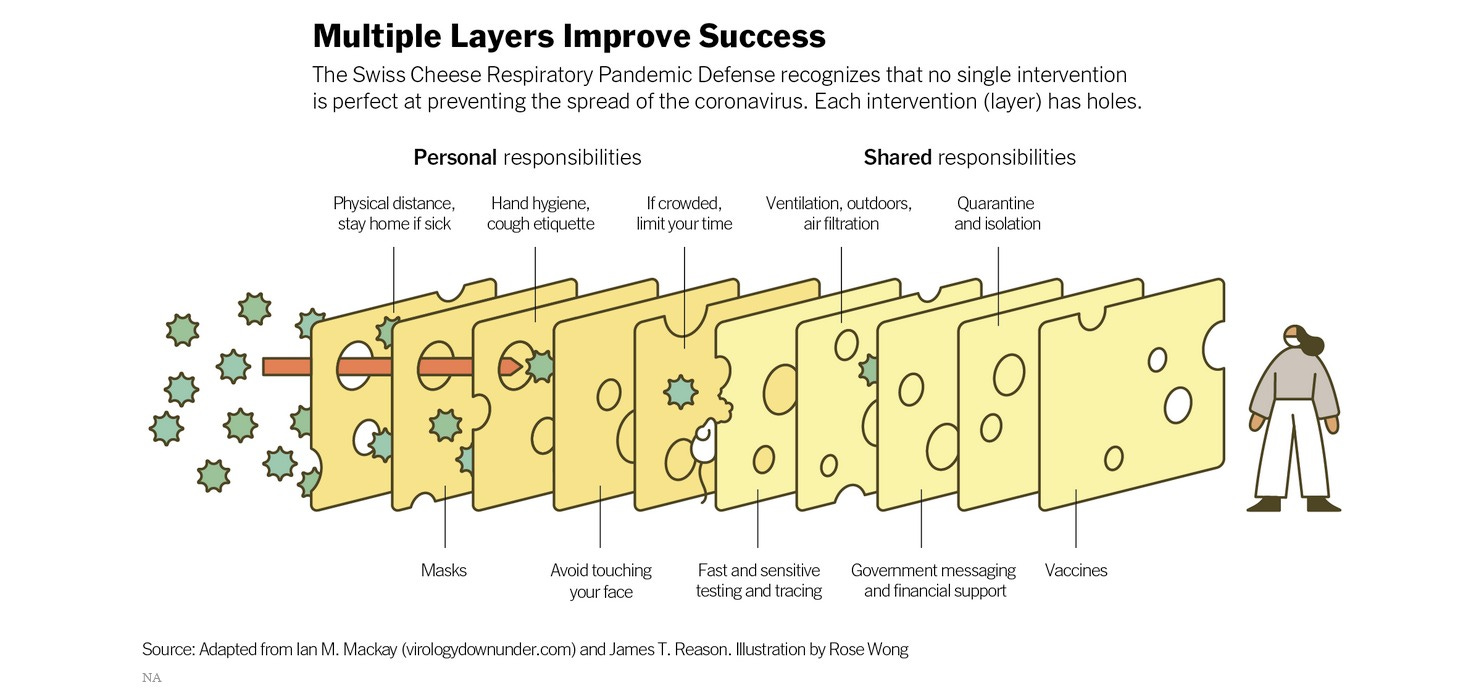
The Swiss Cheese Model of public health pandemic mitigations is supposed to demonstrate the need to use all safe & effective tools available because none are guaranteed perfect, all have weaknesses, so you use them all together to reap the benefits of the barrier created by the collective implementation.1
The swiss cheese does NOT represent an à la carte menu.
Viewing the Swiss Cheese Model of multiple layers of interventions as an à la carte menu is a gross misunderstanding of public health strategy. And any interpretation of multiple measures as a design your own combo meal misses the complexity of this strategy entirely.
Anyone thinking in these simplistic smorgasbord terms, claiming you can just do some kind of pick and choose one or two is just wish casting and should not be trusted for evidence based advice on personal protection or public safety.
When there is a virus circulating and there are little or no other mitigations in place, wearing a well fitting respirator mask is the primary protection an individual can implement. Anti-mask pressure is irrelevant to reality. Claiming you can just pick some other two measures and hope that it takes the place of masking would be like a motorist claiming they don’t need a seatbelt because their car is enhanced with airbags or they think that their fellow licensed drivers might be rational actors who will surely voluntarily stop at intersections through self realized individual agency even without stop signs or laws. We need All The Things for traffic safety. And if someone suggested they didn’t need brakes on their car because there’s a hill they could roll up to stop on in their geographical community, we would not consider this a rational person.
There’s no individualized combo platter approach where randos just pick and choose a couple measures they fancy today to make an à la carte safety scheme. That just wouldn’t lead to overall safety or successful outcomes on the highways. The same is true of infection control measures and stopping the spread of disease. We need public health regulation.
I know this is difficult to deal with in the current political climate where ideologues keep insisting that you can self-actualize yourself out of risk and win the zombie apocalypse if you’re smart, but that’s bullshit based on fantasies. There is no invisible force of self-regulation that will come finally to convince everyone, that should be obvious by now. There has been no miracle for traffic safety, just layers of safety features and regulations working together. There will be no tipping point where people just “wake up” - this is apocalyptic hopium pushed dishonestly by people who want to slow or stop government regulation by keeping people inactive waiting for a miracle instead of taking precautions and pressuring for sensible rules and requirements. This is the same bunk that brought you “the invisible hand of the market” and the myth of “rational actors” in rational choice theory. And as Richard Thaler has pointed out, this invisible hand waving is just plain silly.2
Limiting promoted mitigations to only one or two things someone thinks won’t upset the right-wingers or “be political” is not going to lead to individuals successfully avoiding infection or preventing potential consequences, and it won’t lead to stopping community spread either. It just leaves the door open to pandemic profiteers with dubious unproven products who target the market of people casting about for some silver bullet. Nose sprays are not a proven covid prevention layer,3 and some products could potentially be harmful or adulterated because they’re being sold without or against regulations and may have dubious quality control, or are on the FDA import alert list.4 And some things, like UV products, should not be attempted DIY, or are not ready for prime time, or may have dubious quality control or untested or untestable claims.5 There are tried and true mitigations we already know about. The anti-vax hysteria and anti-mask panic, and their accompanying pseudoscience fads and hype cycles will go down in history as ridiculous. Those catering to that nonsense will be viewed in history much like we view the fringe who perpetrated the Salem witch trials (which occurred after a smallpox outbreak),6 and the few wealthy merchants who made history with Tulip craze nonsense (at the time of an outbreak of plague).7
At the time of ongoing waves of flu outbreaks following the 1918 flu pandemic, Warren G. Harding ran for president in 1920 with “return to normalcy” as his slogan,8 so denial and motivated reasoning is nothing new. But in 1928, James A. Tobey wrote in the American Journal of Public Health and urged people to write their representatives and senators to support a public health science bill saying, “It would be helpful if sanitarians would communicate with their United States Senators and Representatives regarding this important matter. Do it now.”9 And began a time of public health research, epidemiology, and disease control measures greatly expanded because “From Roosevelt’s New Deal in the 1930s through Johnson’s Great Society of the 1960s, a federal role in services affecting the health and welfare of individual citizens became well established.”10
Public health and regulation. Brought about by political pressure. Times have changed. The future is now. But public health must be tended to because it is not a set it and forget it system, and it will not be delivered to us on an à la carte combo platter.
Write your reps. Do it now.
References:
The New York Times – The Swiss Cheese Model of Pandemic Defense. It’s not edible, but it can save lives. The virologist Ian Mackay explains how. By Siobhan Roberts – Published Dec. 5, 2020 – Updated Dec. 7, 2020 No one layer is perfect; each has holes, and when the holes align, the risk of infection increases. But several layers combined — social distancing, plus masks, plus hand-washing, plus testing and tracing, plus ventilation, plus government messaging — significantly reduce the overall risk. Vaccination will add one more protective layer. “Pretty soon you’ve created an impenetrable barrier, and you really can quench the transmission of the virus,” said Dr. Julie Gerberding, executive vice president and chief patient officer at Merck, who recently referenced the Swiss cheese model when speaking at a virtual gala fund-raiser for MoMath, the National Museum of Mathematics in Manhattan.
PBS Hacking Your Mind Weapons of Influence Episode 102 Aired: 09/16/20 Thaler helped to create a new field, behavioral economics, for which he won the Nobel Prize. One of the field’s key insights is that gut feelings like loss aversion lead consumers to make predictable mistakes, and companies in a market economy make a lot of money by encouraging us to make those mistakes. Until then, the widely accepted view had been that markets actually protect consumers from their mistakes.Thaler: “And so I would often hear something like the following — “Yes, yes.I understand that the people in your experiments and some of the people I know do foolish things, but in markets, then — and then I claim…” They could never quite finish this sentence without literally waving their hands, and the argument is somehow if you choose the wrong career or fail to save for retirement, that the market will somehow push you back toward being rational. There’s a reason why no one can make this argument without waving their hands, and that’s because the argument is just silly. You know, if you don’t save enough for retirement, what happens to you? You’re poor when you’re old. The market doesn’t discipline you.
Arznei-telegramm – BEWARE MISINFORMATION – VIRX (other trade names: ENOVID, FABISPRAY): Nasal spray to combat COVID-19? Over 30% of the randomised subjects were subsequently excluded from the study due to a negative PCR test result and only “high-risk” patients (42% to 45% of the individuals initially randomised) were deemed eligible for the principal analyses (5). The 75% reduction in the risk of infection, as claimed, stems from a retrospective observational study conducted in Thailand (2,3). The latter has not been published and cannot, therefore, be assessed. Furthermore, no benefits can be confirmed on the basis of this study due to its inappropriate design. Since nitric oxide is presented as effective active principle that allegedly destroys viral integrity (3,5), we do not believe that the spray can be justifiably marketed as a medical device. Just one month ago, the French Medicines Agency, ANSM (French National Agency for the Safety of Medicines and Health Care Products) pointed out that antiviral nasal sprays with an essentially pharmacological effect are to be classified as medicinal products in Europe (6). Upon request, the competent German regional authority informed us that the marketability of the nasal spray as a medical device is currently under investigation (7).
US FDA – Import Alert 66-41 Unapproved new drugs present public health and safety risks because they have not been reviewed by FDA for safety or effectiveness. Without FDA review, there is no way to know if these drugs are safe and effective for their intended use, whether they are manufactured in a way that ensures consistent drug quality, or whether their labels are complete and accurate. Unapproved new drugs have resulted in patient harm, and the agency works to protect patients from the risks posed by these drugs.
A Precautionary Path with Kaitlin Sundling, MD, PhD – Safer air needs proven technology – Don’t fall prey to misleading claims – proven methods of HEPA filtration and ventilation can reduce viral risk as part of a multilayered approach – OCT 2, 2023 UVC can cause severe skin and eye burns (corneal damage known as photokeratitis) with unprotected exposure. On the SUNY Geneseo campus in January 2022, UVC lamps were installed in classrooms in an attempt to reduced COVID risks. The UVC lamps were inappropriately installed with the UV light source visibly exposed, causing skin and eye burns for multiple faculty members.9 Given the above considerations, any exposed UV light source should be considered unsafe and should be avoided. Far-UVC is an emerging technology that uses light centered at 222 nm. This approach has been promoted with insufficiently supported claims that the 222 nm wavelength of UV light is safe for human exposure while inactivating viral particles. Far-UVC devices do NOT have well-established safety or efficacy. Long term follow up is particularly limited in existing studies of the safety of Far-UVC. It is also difficult to know what wavelengths of UV light are being emitted by a device unless a company publishes their spectral power distribution.10
Library of Congress – Witchcraft in Salem – On March 1, 1692, Salem, Massachusetts authorities interrogated Sarah Good, Sarah Osborne, and an Indian slave, Tituba, to determine if they indeed practiced witchcraft. So began the infamous Salem Witch Trials of 1692 A recent epidemic of small pox, heightened threats of Indian attack, economic uncertainties, and small town rivalries may have all primed the people of Salem and its surrounding areas for the mass hysteria that fueled the witchcraft trials.
Tulip mania: the classic story of a Dutch financial bubble is mostly wrong – Published: February 12, 2018 – Anne Goldgar And what of the much-vaunted effect of the plague on tulip mania, supposedly making people with nothing to lose gamble their all? Again, this seems not to have existed. Despite an epidemic going on during 1636, the biggest price rises occurred in January 1637, when plague (mainly a summer disease) was on the wane. Perhaps some people inheriting money had a bit more in their pockets to spend on bulbs. Prices could be high, but mostly they weren’t. Although it’s true that the most expensive tulips of all cost around 5,000 guilders (the price of a well-appointed house), I was able to identify only 37 people who spent more than 300 guilders on bulbs, around the yearly wage of a master craftsman. Many tulips were far cheaper. With one or two exceptions, these top buyers came from the wealthy merchant class and were well able to afford the bulbs.
Return to normalcy - From Wikipedia "Return to normalcy" was a campaign slogan used by Warren G. Harding during the 1920 United States presidential election. Harding would go on to win the election with 60.4% of the popular vote. 1920 election. In a speech delivered on May 14, 1920, Harding proclaimed that America needed "not nostrums, but normalcy".[1] Two months later, during a homecoming speech, Harding reaffirmed his endorsement of "normal times and a return to normalcy."[2] World War I and the Spanish flu had upended life, and Harding said that it altered the perspective of humanity. He argued that the solution was to seek normalcy by restoring life to how it was before the war.[3] Harding's conception of normalcy for the 1920s included deregulation, civic engagement, and isolationism.[3] He rejected the idealism of Woodrow Wilson and the activism of Roosevelt, favoring the earlier isolationist policy of the United States.[4]
American Journal of Public Health – LAW AND LEGISLATION – JAMES A. TOBEY, LL. B., DR. P. H. Pass the Parker Bill – 1928 (NIH.gov) Pass the Parker Bill-A vigorous resolution urging Congress to pass the Parker Bill for federal health coordination over the veto of the President was adopted by the Association at its 57th Annual Meeting in Chicago in October, 1928. The second session of the Seventieth Congress convenes December 3, 1928, and will adjourn March 3, 1929. The time for action is short, but there is time enough for this desirable procedure. The principles of the Parker Bill have been indorsed by the American Public Health Association every year since 1925, and Congress finally adopted the measure, somewhat amended, in May, 1928. Apparently due to the influence of General H. M. Lord, Director of the Budget, President Coolidge vetoed the bill on May 18, giving as reasons the fact that one section was considered unconstitutional and that the bill tended to ” militarize ” the U. S. Public Health Service. The palpable fallacies of these arguments have already been discussed in this department. Though the Parker Bill by the amendments lost a certain effectiveness, it is still a very important measure, especially in its provisions for allowing the detail of U. S. Public Health Service personnel to other government bureaus; in granting a commissioned status to sanitary engineers and other scientific personnel of the service; in providing for a Nurse Corps; and in setting up a national advisory health council. Sanitarians are still interested in this excellent measure and keenly desirous that it be passed now. If it is not, the bill must be reintroduced and passed all over again in the next Congress. It would be helpful if sanitarians would communicate with their United States Senators and Representatives regarding this important matter. Do it now.
Institute of Medicine (US) Committee for the Study of the Future of Public Health. The Future of Public Health. Washington (DC): National Academies Press (US); 1988. 3, A History of the Public Health System. Available from: https://www.ncbi.nlm.nih.gov/books/NBK218224/ From the 1930s through the 1970s, local, state, and federal responsibilities in health continued to increase. The federal role in health also became more prominent. A strong federal government and a strong government role in ensuring social welfare were publicly supported social values of this era. From Roosevelt’s New Deal in the 1930s through Johnson’s Great Society of the 1960s, a federal role in services affecting the health and welfare of individual citizens became well established. The federal government and state and local health agencies took on greater roles in providing and planning health services, in health promotion and health education, and in financing health services. The agencies also continued and increased activities in environmental sanitation, epidemiology, and health statistics. Federal programs in disease control, research, and epidemiology expanded throughout the mid-twentieth century. In 1930, the National Hygienic Laboratory relocated to the Washington, D.C., area and was renamed the National Institute of Health (NIH). In 1937, the Institute greatly expanded its research functions to include the study and investigation of all diseases and related conditions and the National Cancer Institute was established as the first of the research institutes focused on particular diseases or health problems. By the 1970s NIH grew to include an Institute for Neurological and Communicative Disorders and Stroke, an Institute for Child Health and Human Development, an Institute for Environmental Health Sciences, and an Institute of Mental Health, among others. In 1938, Congress passed a second venereal disease control act, which provided federal funds to states for investigation and control of venereal diseases. In 1939, the Federal Security Agency, housing the Public Health Service and national programs in education and welfare, was established. The Public Health Service also continued to expand. During World War II, the Center for Disease Control was established, and shortly thereafter, the National Center for Health Statistics. (Hanlon and Pickett, 1984) Federal programs supporting individual health services and state programs also continued to grow, both in number of health problems and types of citizens addressed. The Social Security Act was passed in 1935. One title of the act established a federal grant-in-aid program to the states for establishing and maintaining public health services and for training public health personnel.