


Yes, Paxlovid is recommended for covid and the science says it works pretty well.
So let’s not get distracted by confused people, including doctors, repeating misinformation.
The NIH Covid19 treatment management page links1 to the CDC explanation of underlying conditions,2 and recommends treatments including Paxlovid,3 for “people with certain medical conditions”4 - which includes being over 50 years old, or being unvaccinated, and also includes a plethora of various diagnosis types.
CDC - COVID-19 Treatments and Medications - Updated Dec. 21, 2023 (archived link)
If you have COVID-19 and are more likely to get very sick from COVID-19, treatments are available that can reduce your chances of being hospitalized or dying from the disease. Medications to treat COVID-19 must be prescribed by a healthcare provider or pharmacist and started within 5–7 days after symptoms appear. Contact a healthcare provider right away to determine if you are eligible for treatment, even if your symptoms are currently mild. Don’t delay: Treatment must be started within 5–7 days of when you first develop symptoms. People who are more likely to get very sick include
older adults (ages 50 years or older, with risk increasing with age),
people who are unvaccinated or are not up to date on their COVID-19 vaccinations,
and people with certain medical conditions, such as chronic lung disease, heart disease, or a weakened immune system.
Some doctors go against clinical indications when it comes to covid.
I’ve been hearing a lot about people who are reporting that doctors are telling their elderly family members not to get Paxlovid. In some cases it’s a radiologist just giving armchair advice to family members based probably on their right-wing social media consumption. But in most cases I’m hearing that people are getting this advice - not to take Paxlovid, from their own doctors, who ought to know better. In almost all these stories I’ve heard about people being denied Paxlovid they want, or being told they don’t need Paxlovid, or sometimes very wrongly that Paxlovid is bad, it’s almost exclusively senior citizens who are being turned down! This is incredibly egregious and scary since being a senior citizen is a primary risk factor for serious covid, complications, hospitalizations, and death.
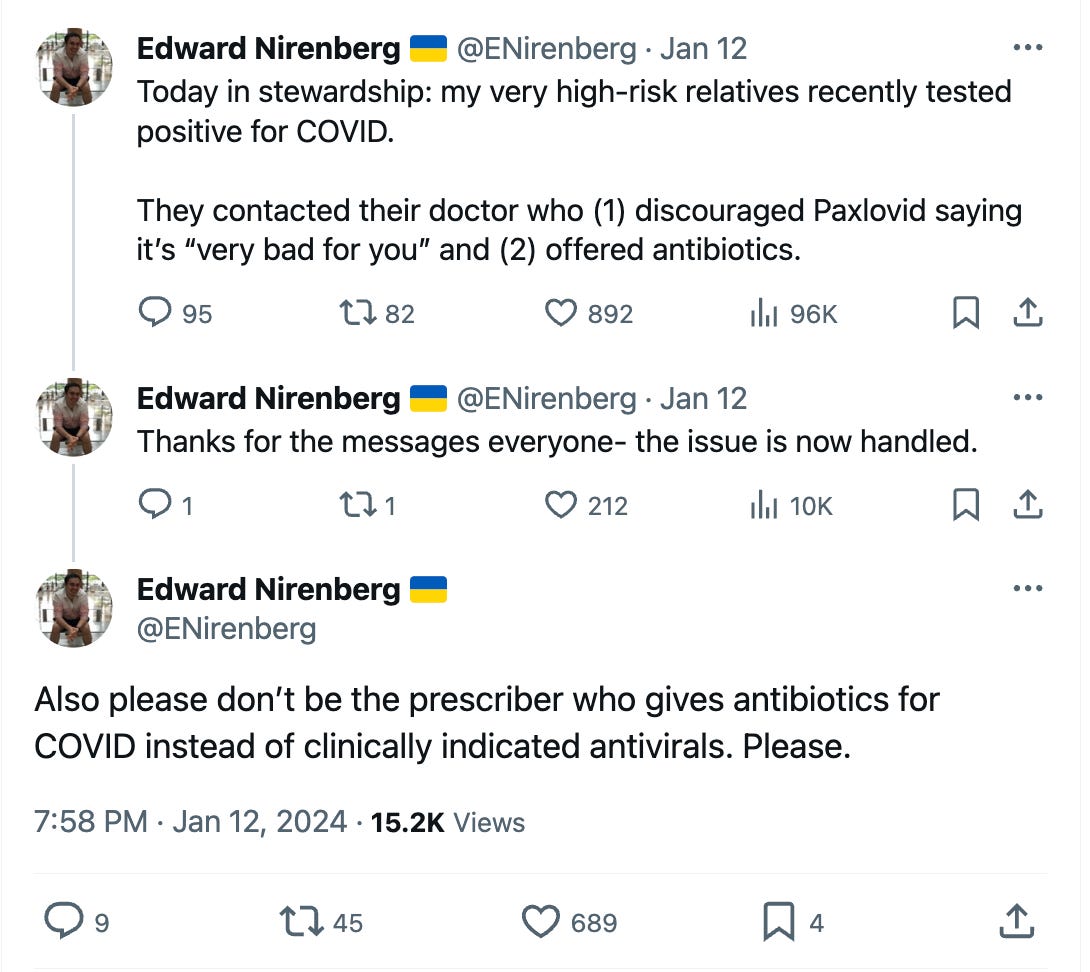
In some of these cases it’s pretty clear the doctors are right-wingers who are thoroughly right-wing QAnon wellness guru social media influencer pilled because they’re recommending specifically z-pack - an antibiotic for bacterial infections, NOT viruses like covid,5 and which has been on a bunch of right-wing covid contrarian anti-vax “covid protocol” treatment text documents passed around on social media since 2020, that also included ineffective hydroxychloroquine that cost some patients their lives.6
In other cases it’s not clear if the doctors are misguided or ignorant. But whatever is going on the government really needs to step in and up the public information, especially for prescribing doctors who are endangering patient lives. Reckless social media consumption is also a problem among ordinary people who are neither anti-vax covid contrarians nor right-wingers. None of us are entirely immune to disinformation operations and PR propaganda, especially if we see it a lot, because of the Mere Exposure Effect.7
There are clinical instructions for doctors on how to prescribe to people on statins.
When it comes to drug interactions, yes the list is long, but some drugs can merely be discontinued during the Paxlovid treatment. A persistent myth is that people can’t ever take Paxlovid if they’re taking any statin (common medication for cholesterol), and that’s simply not how it works. I don’t understand how this is not common knowledge 2 years later. I heard about this option from the get-go, or at least as far back as when Eric Topol first blogged about Paxlovid in December 2021.8 Almost a year later in November 2022, I actually recalled Doctor Topol mentioned that he himself would be suspending his statin to take Paxlovid were he to get covid.9 And by that time I’d heard from multiple doctors of family members that they just prescribed Paxlovid with the instruction to discontinue the statin while on Paxlovid, or for a week or whatever. I assumed this was in some standard treatment instructions that doctors read about the interactions when prescribing stuff. (Clearly not all doctors though!) Most of the older people I personally know who’ve had covid have been getting Paxlovid for the past 2 years. Granted, mostly educated middle class people or upper middle class professionals, or living in “blue states” etc. We know probably all the upper echelon in the government takes this drug because they often mention it in the news, from President Joe Biden,10 to MSNBC’s Chris Hayes.11 You can’t tell me that a lot of these people are not on statins, like the people in Congress, some who my local Rep. Matt Cartwright, had described as “elderly” and “not too spry” when describing needing to rush down the steps to the basement during the insurrection at the capitol.12 One 88 year old Republican Senator retired because of long covid, and said that he knew of others who have long covid but don’t admit it publicly.13 And that’s because they’re not masking, they’re gathering all the time, and they’re not being careful, so they’re getting covid, and it’s reasonable to assume they’re getting Paxlovid, many who take statins. I’m not saying that I know whether or not Doctor Fauci or Bernie Sanders or Nancy Pelosi are on cholesterol meds, but it’s a widely and commonly prescribed medication among people over 50. (At least middle and upper class people over 50 with decent prescription insurance.) In January 2023, Eric Topol and another doctor, Ashish Jha, who was then the White House COVID-19 Response Coordinator, were on a podcast on Medscape, where they specifically talked about the practice to temporarily suspend statin use in order to take Paxlovid for covid, in the context of hand wringing over the misconceptions involved in the underuse of Paxlovid!14 Obviously this is pretty rich coming from someone (Ashish Jha), who conceivably should’ve been able to do something to make sure there was better information getting out there about Paxlovid. (And covid precautions in general.) Nevertheless, when Eric Topol did unfortunately get covid a year later, in December 2023, he blogged about taking Paxlovid in his newsletter. He doesn’t mention the statin, but men his age rarely stop taking statins they were taking a year ago, so it’s probable he’s still on the statin and did just what he said he was going to do, take the Paxlovid.15 And on January 5th, 2024, Jeremy Faust blogged about the issue of statins and Paxlovid, specifically stating the FDA advises on how to prescribe to patients on the 4 statins with conflicts!16 Doctor Faust links to this FDA checklist tool for prescribers, (that I just knew had to exist), and specifies that with some statins to consider going off for 5 days, others for also an additional 5 days, and for some statins there’s no need to suspend taking them at all because the other 3 statins don’t even have a Paxlovid conflict!
The FDA has a Paxlovid Checklist Tool for Prescribers.
FDA PAXLOVID Patient Eligibility Screening Checklist Tool for Prescribers
HMG-CoA reductase inhibitors (statins)
• If the patient is taking lovastatin or simvastatin, which are contraindicated with PAXLOVID coadministration, PAXLOVID can be given if the statin can be held 12 hours prior to the first dose of PAXLOVID treatment, held during the 5 days of treatment, and restarted 5 days after completing PAXLOVID.
• If the patient is taking atorvastatin or rosuvastatin, consider temporary discontinuation of atorvastatin and rosuvastatin during treatment with PAXLOVID. Atorvastatin and rosuvastatin do not need to be held prior to or after completing PAXLOVID
Doctors should be consulting this prescriber checklist, because renal impairment isn’t always a deal breaker either, depending on the assessment, a dose reduction of Paxlovid might be the answer. And, they should be warning patients, who are not always honest with their doctors about taking supplements - that one of the red zone no way should you mix Paxlovid with this is actually St. John’s Wort.17
Not everyone with high risk conditions knows they’re in the high risk category.
I’ve seen a lot of people online thinking they’re very clever to point out that “young healthy people” don’t need treatment. Strangely some people mistakenly think that means them when it’s not true. I’ve seen a Medicare age senior citizen doctor, simultaneously pointing out he’s in the high risk group of being a senior citizen, and in the same breath claiming he is not in a risk category. Spoiler alert, it’s Bob Wachter, and he even claimed he doesn’t live with anyone at risk, and not to be indelicate, but I’m pretty sure his wife is over 50.18 Even doctors can be in denial of being in the recommended category for some reason. Unfortunately another issue is that there’s a period of time where someone has a condition but hasn’t yet been diagnosed. I’ve heard of people getting diagnosed for the first time with other things when they happen to get hospitalized with covid by surprise because they didn’t think it would be them. People should get their checkups and report symptoms to doctors generally to get diagnosed timely, but there’s always going to be a gap.
Personally I think anyone who has covid should consult a doctor to see about what treatment or course of action is right for them in any case. In many cases, a doctor will tell someone "If this happens head to the hospital" for example. It's a potentially serious disease and nobody should feel awkward seeking medical advice and treatment, including but not limited to Paxlovid. I've never heard anyone say "I'm sorry I mentioned my mole to my doctor a year ago that turned out to be benign" but I have heard people say "I regret not mentioning this unusual mole a year ago when it was more easily treatable cancer" - because there’s always a window of best treatment. With Paxlovid the window is the first few days after testing positive or starting symptoms.
Paxlovid might reduce the risk of Long Covid, but the reduction in risk of death or hospitalization is still the selling point!
Paxlovid has been shown to potentially reduce the risk of post covid conditions,19 like Long Covid. Drugs aren’t approved though on the basis of “they might do something” obviously, but that’s not what’s going on here. Like vaccination, it’s primarily known to reduce the risk of hospitalization and death, and that’s why it is a scientifically valid choice. And frankly, that should be huge for everyone, since even young people are known to sometimes get very sick with covid.20 Unfortunately, people (especially on social media), trying to make the point about it “not stopping” Long Covid or that we don’t know if it has preventative effects, unwittingly I think, wind up sounding like they’re arguing that Paxlovid is ineffective or not worth getting. Yes, even if it does reduce the chances of getting Long Covid, it cannot be depended upon to guarantee you won’t get post-covid complications. But avoiding hospitalization or the grave is still on the table! And there’s apparently enough evidence21 that it helps somehow with Long Covid, that further studies are underway in the U.S. and Sweden to look at using Paxlovid to treat Long Covid.22 Which makes sense since if it reduces severity in other ways, it’s reasonable to think that it might help or reduce the risk of at least some post-covid effects. In the meantime though, it’s been shown to prevent very severe covid, and who doesn’t want that?
The only people panicking about “rebound” are the people in charge of employee schedules.
Another point that seems to get muddled on social media and in the public discourse, including by doctors, is the concept of rebound. Covid rebound is when people start to feel better, then take a turn for the worse, or just start testing positive again after a negative test. This has been reported since the very beginning of the pandemic. Even before Paxlovid there were warnings about people who would appear to be getting better after a few days, and then wind up hospitalized on day 10.23 Recovery from any illness is rarely textbook and linear anyway. But with Paxlovid, this rebound tends to be comparatively mild, and since Paxlovid also prevents hospitalization,24 then it is pretty clear on its face that Paxlovid Rebound is far preferable to Bare Ass Covid Rebound. The NIH’s treatment guidelines specifically state, “To date, the recurrence of COVID-19 symptoms and virus detection following the use of antiviral therapies has not been associated with progression to severe COVID-19. Therefore, concerns about the recurrence of symptoms or viral rebound should not be a reason to avoid using antiviral therapies.”25 Non-hospitalized covid rebound is not worse than dying or hospitalization. And that ought to be the end of the decision making on that point. But there’s been confusion. There’s no evidence Paxlovid actually extends the entire course of illness, in fact the opposite would seem like the logical assumption. But people speculated about CDC Director Rochelle Walensky’s 18 days of “mild” covid with Paxlovid, but even at the time I thought that, for all we know, the alternative without Paxlovid could’ve been 18 days on ECMO, or 18 weeks in pulmonary rehab, or 18 months off work and Long Covid. Nobody could really say so we have irrelevant thesis at best. All we know is that Rochelle Walensky was over 50 when she got covid in October 2022,26 and we later learn that “in the second half of 2022, 97.3% of people who died from Covid in this country were aged 50 and older.”27
But employers panicked at the mention of Paxlovid rebound, terrified that workers would take Paxlovid and need extended sick leave amid labor shortages (ironically probably caused in part by workers pressured to work sick and spread the virus to their coworkers). I wondered if these employers and their PR consultants didn’t give a crap if employees were hospitalized or died, but maybe they weren’t thinking things through, as so often is the case when elites panic.28 And so the PR machine spun up to discourage working people from taking Paxlovid. Also, the supplement influencers, just like they prefer people unvaccinated and feeling unprotected looking for something else to buy for covid, the people selling pseudoscience wares grabbed onto trashing the Paxlovid as well, so people spend a bundle on their dubious remedies instead.29 And also there’s the problem of some healthcare spokespeople doing very poor science communication because they're more interested in hype that will get clicks and dopamine hits on their social media feed30 than giving people usable sensible information. And then that goes through a game of Telephone Gossip repeated unwittingly,31 and it can sound confusing if you’re not giving it your full attention when you’re on autopilot32 doom scrolling. But if you think things through, being sick for a few days and even testing positive for a few more, beats the ever living poop out of being hospitalized and maybe being sick for weeks or more - or worse!
A very niche silo concern I heard related to the theory of Paxlovid Rebound, of which again there’s “no strong evidence that Paxlovid causes” - nevertheless has gotten some people speculating that it’s reason to think there will be some kind of spurred level of viral evolution like the concerns around the covid mutations linked to molnupiravir - but even with that - “The study doesn’t say people should not use molnupiravir but calls for public health officials to scrutinize it.”33 I haven’t seen reason to think this is something to fret about with Paxlovid, but speculating social media hotshots suggest it in passing, then bad actors add this claim in their arsenal to pooh-pooh Paxlovid use. It reminds me of the kind of ridiculous, nonsensical argument that Monica Gandhi, who is frequently proven wrong,34 used to not get the vaccine booster back in 2021, claiming it was out of concern for global vaccine equity, though when Democracy Now reported this, they pointed out that the advisor for Doctors Without Borders pointed out that the issue of global vaccine inequity is caused by global leaders35 - not individuals. And Monica Gandhi’s refused booster shot was not going to be sent to Africa because she turned it down. These are the same kind of upside down woke-washing arguments used by anti-maskers, lockdown revisionists, and climate contrarians.36 And by the same token, it’s rude and misguided form of DARVO (deny, attack, and reverse victim / offender)37 to suggest people are doing some kinda noble sacrifice to refuse Paxlovid because of some mythical potential concern years from now, when your hospitalization with Bare Ass Covid Rebound now could cost other people their lives in an overloaded ER with a treatable emergency right in the present tense. It’s the kind of argument Longermist TESCREAL weirdos make about an eyelash in the eye of a bunch of future humans is more of a concern than a human today suffering unbearable torture, or whatever bonkers and immoral thought experiments they get up to.38
Immunocompromised people should not be villainized for trying to not fall by the wayside.
And wow, then there’s the mixed up arguments by people who think it’s wrong for immunocompromised people to keep Paxlovid on-hand, and call it “hoarding” and unethical. Even Doctor Anthony Fauci admitted to the BBC that going forward, the vulnerable will “fall by the wayside”39 and it’s not wrong for those people to try and avoid falling by the wayside. So it’s not surprising that high risk people have been known to get Paxlovid in advance, typically with their doctor’s care and understanding, so they’re not scrambling to get it when they turn up positive in a surge, when they have difficulty leaving their house, and it may be in short supply. (Probably because of the cost since it was commercialized! so nearby pharmacies won’t stock enough!) And because everyone else has been reckless, and spread the virus so much the high risk person couldn’t avoid but to contract covid at a necessary doctor appointment or something. What's unethical is that doctors sometimes aren't even prescribing it to high risk people, or not prescribing it timely, telling misinformation to patients about it - like that it’s only for severe disease (when it’s to prevent severe disease). Unethical is having people who really tried to not get infected denied Paxlovid because a bunch of rich people rolled the dice partying during a surge and have bought up all the supply. Disease is never fair, and pandemics always involve unappealing situations and behaviour. The problem isn’t disabled people prepping, it’s doctors and other people in charge dropping the damn ball repeatedly, often to cater to business interests like the CDC followed the recommendations of Delta Airlines in December 2021.40
For-profit healthcare is terrible, but it’s also evidence that medicine works, otherwise we wouldn’t care how much they charge.
Another weird idea is that, because Pfizer is a profit seeking crap company, and the U.S. financial system is borked, and industries have outsized influence on the U.S. government, that somehow this translates wrongly into the scientist employees making medicines that are suspect somehow. The Pfizer executive at their earnings call meeting sure sounded greedy and gleeful about seeing masks cast aside so people would get covid and buy more Paxlovid. I sure thought that was ghoulish.41 But it’s not evidence against the scientists and the drug they developed, just because the company lobbies the government for favour to protect their profits.42 The idea that it calls the science into question is ridiculous because we wouldn't care how much they charged for this stuff if it wasn’t so vital. So if you don’t trust a vaccine or Paxlovid from Pfizer, because Corporate America is cruel and counterproductive, by that logic, you’d be wrongly recommending diabetics stop using insulin instead of pushing for it to be more affordable, and you wouldn’t be taking Pfizer’s highly profitable Z-pak43 either!
Spoiler Alert: Doctors are humans with phones that have access to social media.
So the takeaway here is that MOST doctors who would be prescribing Paxlovid will know the patient’s medical history and medications, and or will review those before prescribing Paxlovid. It’s largely up to the doctor to decide to prescribe based on just one risk condition in the list, and there are plenty of doctors who prescribe it on the basis of that, because even one risk condition puts someone in the risk category, and a study in 2021 estimated 75% of American adults have at least one of those risk conditions.44 But it’s also possible doctors don’t keep up with that list, which has been updated over time, or haven’t even looked at the FDA Paxlovid checklist for prescribers. But the key detail here is that if the doctor does not cite a contraindication when denying Paxlovid, and especially if the person is clearly in an obvious high risk category (like over 50 or unvaccinated!), or the doctor claims that Paxlovid doesn’t treat covid or something outlandish, a second opinion can usually be sought and likely should be. Sadly doctors are fallible like anyone else, and they have access to the same cesspool of social media garbage and get caught in the same trashcan silos of noise that the rest of us do. Horrendously some government officials in some countries have been entirely alt-right qanon pilled on covid or are just austerity adherents, and actively stop citizens from getting paxlovid, or at least it’s not easy. (Of course wealthy people anywhere have little problem getting what they want.) Perhaps this trend will change if we can push for better public health messaging, and more media literacy to push back against The Internet of Fakes and all the pandemic profiteering that goes with it.45
Let’s work with the pandemic reality we have, and push for the real mitigation we want.
Like the vaccines, we got a Paxlovid sooner than I’d expected given my expectations in early 2020, especially given the erratic and dysfunctional state of our society today. But it’s not a supernatural miracle pill. Like many medications and medical treatments, with any given intervention, there is always potentially an element of it being A Hail Mary.46 Even the best, most highly effective and proven treatment courses don’t always work out right for everybody. But we don’t withhold cancer treatments for that reason.
Ideally people wouldn’t get covid at all, it would be prevented. But universal masking isn’t even always a thing in healthcare even though many people want that.47 And you can’t wear an N95 mask in the dentist chair, though I think everyone else in the dentist office should be wearing them for that reason.48 Preferably people would be vaccinated, and up to date on their boosts, but while that reduces the chances of transmission for a period, it’s mostly useful for diminishing the effects of infection, beneficial effects of the vaccine wane over time,49 and a boost isn’t a guarantee either. So this is, as always in public health, a layers situation.50 Including Paxlovid - We need all the things.
“Disclosure” (of nothing)
I have no financial relationship with Pfizer other than being a general customer of medications like anyone else. Nobody at Pfizer or any other drug company is paying me to endorse or mention Paxlovid, or anything else, or for any other reason. I’m not seeking direct or indirect payments of any kind from pharmaceutical companies or drugstores. And as far as I know I don’t have any friends or family employed by Pfizer.
In the U.S., bloggers and social media influencers, etc, are required by law to disclose when paid to promote a commercial product or service.51 It’s true sometimes people don’t disclose, and in some cases get in substantial trouble with the SEC52 — but that seems really dicey to me, and I’m pretty risk averse so if I were to do marketing of any type, I’d be complying with the FTC,53 and I personally think everyone ought to disclose when they’re being paid to promote something, whatever it is.
References:
NIH COVID-19 Treatment Guidelines Clinical Management of Adults Summary Last Updated: October 10, 2023 Patients Who Are at High Risk of Progressing to Severe COVID-19b,c Preferred therapies. Listed in order of preference: Ritonavir-boosted nirmatrelvir (Paxlovid)d (); see footnote on drug interactionse Remdesivird,f () Alternative therapy. For use when the preferred therapies are not available, feasible to use, or clinically appropriate: Molnupiravird,g,h ()
CDC - COVID-19 - Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19: Information for Healthcare Professionals - Updated Feb. 9, 2023 An updated list of high-risk underlying conditions, along with their associated evidence, is provided below. The conditions are grouped by the level of evidence, with the highest level shown in the top section. The list of underlying medical conditions is not exhaustive and will be updated as the science evolves. CDC continually reviews additional underlying conditions, and some of these might have sufficient evidence to be added to the list. This list should not be used to exclude people with underlying conditions from recommended measures for prevention or treatment of COVID-19.
CDC - COVID-19 Treatments and Medications - Updated Dec. 21, 2023 FDA has authorized or approved several antiviral medications used to treat mild to moderate COVID-19 in people who are more likely to get very sick. Antiviral treatments target specific parts of the virus to stop it from multiplying in the body, helping to prevent severe illness and death.
CDC COVID-19 - People with Certain Medical Conditions - Updated Feb. 10, 2023 This means that a person with one or more of these conditions who gets very sick from COVID-19 (has severe illness from COVID-19) is more likely to: - Be hospitalized, - Need intensive care, - Require a ventilator to help them breathe, - Die
Oldenburg CE, Pinsky BA, Brogdon J, et al. Effect of Oral Azithromycin vs Placebo on COVID-19 Symptoms in Outpatients With SARS-CoV-2 Infection: A Randomized Clinical Trial. JAMA. 2021;326(6):490–498. doi:10.1001/jama.2021.11517 Findings In this randomized trial that included 263 participants with SARS-CoV-2 infection, treatment with a single oral dose of azithromycin, 1.2 g, vs placebo resulted in self-reported absence of COVID-19 symptoms at day 14 in 50% vs 50%; this was not statistically significant. Meaning Among outpatients with SARS-CoV-2 infection, treatment with a single dose of oral azithromycin compared with placebo did not result in a greater likelihood of being free of symptoms at day 14.
Futurism - 17,000 People Died From Taking Hydroxychloroquine, Scientists Estimate Patients were basically guinea pigs. January 5, 2024 / by Sharon Adarlo In news that's sure to kickstart a wave of recriminations, researchers have estimated that almost 17,000 people died in six countries during the first COVID-19 wave due to the use of hydroxychloroquine (HCQ), an anti-malaria medication that gained viral traction as a potential treatment against COVID even after scientific evidence failed to back up its efficacy. A team of researchers from France, Canada and China revealed the findings in a new study published in the science journal Biomedicine & Pharmacotherapy. They arrived at the number after performing statistical analysis on medical and hospital data about excess mortality. "During the first wave of COVID-19, hydroxychloroquine (HCQ) was used off-label despite the absence of evidence documenting its clinical benefits," the researchers write. "Since then, a meta-analysis of randomised trials showed that HCQ use was associated with an 11 percent increase in the mortality rate."
Mere Exposure Effect CHLOE HUMBERT JAN 1, 2024 After repeated exposure to something it becomes familiar, and even if it’s false or bad, it can come to be viewed as true or acceptable - even favorable, simply because it feels familiar.
Ground Truths - Why Paxlovid is a Just-in-Time Breakthrough The first potent anti-Covid pill will be a big help ERIC TOPOL DEC 16, 2021 This works through a cytochrome (3A4) that is in common with the metabolism of many frequently used drugs such as statins and certain blood thinners, so a temporary 5-day off such drugs, or adjustment of their doses may be appropriate or necessary.
Ground Truths - Paxlovid and Long Covid - A new study sheds light on a bonus benefit after the acute phase - Eric Topol Nov 6, 2022 Last point. Until we have more data, I believe the body of evidence should make us treat more with Paxlovid to derive both acute and longer-term benefits. I have not had Covid, but if I do get it, I will be certain to take Paxlovid, temporarily stop my statin for 5-days. I will also be treating my patients with Paxlovid more liberally with knowledge of the new report.
The Morning Call - U.S. Rep Matt Cartwright describes House members escape amid capitol breach. January 6, 2021 Then, police ordered members toward a stairwell in the chamber’s southwest corner where narrow and steep stairs lead to basement tunnels all over the Capitol. “That’s when it started to feel a little dicey because some of our members, they’re elderly and they’re not too spry,” he said. As members descended, a police officer ordered them to move faster yelling, “They’re right behind us,” he said.
Business Insider: Former GOP Senator James Inhofe retired because of long COVID symptoms. Other colleagues have it but keep it secret, he said. by Isobel van Hagen Feb 26, 2023 He said "five or six" other political colleagues have long COVID, "but I'm the only one who admits it." Inhofe left office before the end of his term last February, and Senator Markwayne Mullin took his place. The 88-year-old repeatedly voted against COVID protections for Americans during his time in office. In March 2020, Inhofe voted against the Families First Coronavirus Response Act, which broadly expanded benefits for those affected by the pandemic. In 2021, he also voted against the American Rescue Plan — which included a $1,400 stimulus check, improved vaccine distribution, and extended unemployment benefits. He did, however, vote in favor of the CARES Act — which offered a $1,200 stimulus check — and generally offered conflicting opinions on the pandemic during his time in office.
White House COVID Chief on Why Paxlovid Is Underused Eric J. Topol, MD; Ashish K. Jha, MD, MPH Disclosures January 31, 2023 - Medscape They had over 1500 respondents. Number one on the list was fear of drug interactions. There's a lot of data to suggest that for the vast majority of drugs, there are no interactions of concern because you can just stop the statin or other medication for 5 days.
Ground Truths A Covid Update ERIC TOPOL DEC 16, 2023 I tested positive and started a prescription for Paxlovid soon thereafter. I had 2 days of marked fatigue, but was otherwise unaffected. Like most of you who have taken it, Paxlovid induced a bad metallic taste, but fortunately I didn’t experience other side effects.
Inside Medicine - Paxlovid or your statin? Patients on some medications are sometimes told they can't take Paxlovid. Is that the right move? Jeremy Faust, MD Jan 5, 2024 First, if you take any statin other than lovastatin, simvastatin, atorvastatin or rosuvastatin, the answer is easy. If you have high-risk conditions for Covid, you can add Paxlovid on top of those other statins without concern for any unsafe interactions. But what if you take lovastatin (Altoprev), simvastatin (Zocor), atorvastatin (Lipitor) or rosuvastatin (Crestor)? Pfizer says that its drug Paxlovid can have drug-drug interactions with these medications, and that the combination could lead to unsafe muscle breakdown. That in turn could lead to kidney problems or even death (albeit that is exceedingly rare). Accordingly, the FDA advises patients to stop taking their lovastatin or simvastatin 12 hours before the first dose of Paxlovid, and to resume the statin 5 days after they’ve completed the 5-day antiviral course. For atorvastatin and rosuvastatin, the contraindication is less strong and the FDA says that clinicians should “consider” temporary discontinuation of these drugs, but only during the 5 days when Paxlovid is being taken.
FDA PAXLOVID Patient Eligibility Screening Checklist Tool for Prescribers HMG-CoA reductase inhibitors (statins) • If the patient is taking lovastatin or simvastatin, which are contraindicated with PAXLOVID coadministration, PAXLOVID can be given if the statin can be held 12 hours prior to the first dose of PAXLOVID treatment, held during the 5 days of treatment, and restarted 5 days after completing PAXLOVID. • If the patient is taking atorvastatin or rosuvastatin, consider temporary discontinuation of atorvastatin and rosuvastatin during treatment with PAXLOVID. Atorvastatin and rosuvastatin do not need to be held prior to or after completing PAXLOVID
Bob Wachter @Bob_Wachter Dec 18 2023 ...had Covid in the past 10 weeks, I wouldn’t don my mask. After 10 weeks, though, that infection or vax doesn’t really help block transmission (though it continues to lower the odds of a severe case & Long C), so I’m back to making decisions based on prevalence only. (16/25) 7) All of this is based on my personal status: a relatively healthy 66-year-old who doesn’t live with anyone vulnerable. I’d be more careful if I was 80, immunosuppressed, or living with someone in either of these categories. And I might be a bit less careful if I was 40. (17/25)
Xie Y, Choi T, Al-Aly Z. Association of Treatment With Nirmatrelvir and the Risk of Post–COVID-19 Condition. JAMA Intern Med. 2023;183(6):554–564. doi:10.1001/jamainternmed.2023.0743 Meaning In people with SARS-CoV-2 infection and at least 1 risk factor for progression to severe COVID-19 illness, treatment with nirmatrelvir during the acute phase of COVID-19 was associated with reduced risk of PCC.
The Conversation - Younger adults can get very sick and die from COVID too. Here’s what the data tell us Published: August 6, 2021 2:50am EDT Age is not the only factor that influences outcomes with COVID-19. Having a chronic illness is associated with higher likelihood of more severe disease and death. Being male and being obese also increase the risk of dying from COVID-19. Obesity may in fact add more significantly to the risk of serious disease in younger people. Of course, none of these risk factors have to be present for a person to develop severe COVID-19.
Ground Truths Paxlovid and Long Covid A new study sheds light on a bonus benefit after the acute phase ERIC TOPOL NOV 6, 2022 Subsequently, there have been many clinical effectiveness studies throughout the world which have not only confirmed this high level of protection from hospitalizations and deaths, but many, such as this one from Israel, showed the partitioning of acute phase benefit by age, not seen in people younger than age 65. There was also the Hong Kong matched pair study of Paxlovid indicating a 66% reduction of all-cause mortality in people age 65 and older (just 17% were < age 65 in that study). Side note: we don’t have many interventions in medicine that achieve this level of proportionate all-cause mortality reduction.
NBC NEWS - Paxlovid may reduce the chance of long Covid. Why don’t doctors prescribe it more? Experts who study and treat long Covid agree that Paxlovid seems to lower the risk of lingering symptoms. Some long Covid patients regret not taking it. Oct. 12, 2023, 9:21 AM EDT By Aria Bendix Studies at the Yale School of Medicine and Karolinska Institutet in Sweden are also investigating Paxlovid as a potential long Covid treatment. Dr. Benjamin Abramoff, director of the Post-COVID Assessment and Recovery Clinic at Penn Medicine, said he recommends Paxlovid for people with long Covid who get reinfected. “I’ve had a couple patients report improvement through that process,” he said. “Even if they’re not necessarily high risk, I think there’s a lot of benefit for many of our patients who have significant long Covid symptoms.”
New York Times - Why Days 5 to 10 Are So Important When You Have Coronavirus Tracking your daily symptoms can help you and your doctors make better decisions about whether a hospital visit is needed. By Tara Parker-Pope Published April 30, 2020 While every patient is different, doctors say that days five through 10 of the illness are often the most worrisome time for respiratory complications of Covid-19, particularly for older patients and those with underlying conditions like high blood pressure, obesity or diabetes. Younger patients who develop complications may begin struggling a little later, as late as days 10 to 12. Most people who reach day 14 without any worrying symptoms (other than feeling miserable and fatigued) are likely to be on the road to recovery. “With any other disease, most people, after a week of symptoms, they’re like ‘OK, things will get better,’” said Dr. Leora Horwitz, associate professor of population health and medicine at N.Y.U. Langone Health. “With Covid, I tell people that around a week is when I want you to really pay attention to how you’re feeling. Don’t get complacent and feel like it’s all over.”
Yale Medicine - What Is Paxlovid Rebound? 9 Things to Know. Whether or not you take Paxlovid for COVID, symptoms can return, but they tend to be brief and mild. BY KATHY KATELLA OCTOBER 9, 2023 Nobody knows for sure how common it is, and there is no strong evidence that Paxlovid causes it—a rebound has been reported by people who took the drug and those who didn’t. Because of this, the Centers for Disease Control and Prevention (CDC) calls the phenomenon “COVID-19 rebound” or, informally, "COVID rebound." Scott Roberts, MD, a Yale Medicine infectious diseases specialist, is concerned less about the rebound than he is about how the phenomenon might affect people’s perception of Paxlovid, the first-line treatment for preventing severe illness from COVID-19. “People may avoid Paxlovid out of a fear of COVID rebound,” Dr. Roberts says. “But for high-risk patients, the benefits of Paxlovid in preventing severe disease, hospitalization, and death far outweigh the downsides of a rebound, which is usually mild, and, in most instances, will do nothing more than prolong the isolation period.”
NIH - COVID-19 Treatment Guidelines - Therapeutic Management of Nonhospitalized Adults With COVID-19 Last Updated: November 2, 2023 To date, the recurrence of COVID-19 symptoms and virus detection following the use of antiviral therapies has not been associated with progression to severe COVID-19. Therefore, concerns about the recurrence of symptoms or viral rebound should not be a reason to avoid using antiviral therapies.
Stat News: FDA offers radio silence on question of spring Covid boosters, as other countries push ahead By Helen Branswell March 16, 2023 Michael Osterholm, director of the University of Minnesota’s Center for Infectious Disease Research and Policy, would go further, saying people who are 50 and older in the U.S. should be offered the chance to get a second booster. He noted that in the second half of 2022, 97.3% of people who died from Covid in this country were aged 50 and older.
Elite Panic. Big shots have different goals than the rest of us. Politicians should be representatives, businesses shouldn’t lead, even billionaires can’t seem to buy common sense, and tech won’t save us. CHLOE HUMBERT JUL 13, 2023 People in charge, politicians and corporate leaders, default to elite panic. Their focus turns to “controlling the public, rather than on addressing the disaster itself” and when a corporation is involved in something bad that happens,”often its first move is not to deal with the actual problem, but to manage the negative perception caused by that problem.” People with power have different priorities - chiefly, maintaining their own power.
MIT Initiative on the Digital Economy - Thinker-Fest: Session 1 - Fireside Chat - How to Fix the “Splinternet” Mar 3, 2023 They are really invested in gaining social capital and reputation for participating in these types of industries. And they also have economic models at play. You can buy flat earth sweatshirts, you can buy anti-vax stickers and notebooks, you can pay subscription fees, you can watch videos that are monetized on YouTube. And this is also very much a reputational economy. We also have a factor that I don't think is talked about a lot which are intentional antagonists otherwise known as trolls. What's interesting about them from a digital community perspective is that they too are chasing social currency but the reputation that they're cultivating within their own communities is one where the more chaos they create, the more reputation credibility that they have. And so these three forces are kind of at play when we look at what's happening from an individual and community's perspective. The issue is that if you broaden out, you start to see that all of these dynamics can take place because there are very clear revenue models and businesses. People are making money from this. For example I trace what's called direct benefits. So these are companies that are selling products and services directly related to the idea that's circulating. So if you are anti-vax, you are selling supplements right, if you are, you're selling essential oils, you're selling products that are directly benefiting from the disinformation or misinformation that is circulating.
Repeat the truth, don't lead with a lie The "truth sandwich" means leading with the facts and repeating the correct information. It's probably the only way to debunk lies without helping to promote them. CHLOE HUMBERT OCT 14, 2022 Even famous scientists, serious doctors, and experienced educators sometimes fall into bad communication habits on social media. These pitfalls are alarming. And I can’t help but notice the adversaries pushing lies never seem to mess this up. They lead with whatever they want you to believe and put it on repeat. They aren’t promoting their opposition, but they are experts in getting hate followers and rage clicks for loads of engagement for themselves.
Sharing of misinformation is habitual, not just lazy or biased, Gizem Ceylan, Ian A. Anderson, and Wendy Wood, Edited by Susan Fiske, Princeton University, Princeton, NJ; received September 28, 2022; accepted December 3, 2022, January 17, 2023 120 (4) e2216614120 Why do people share misinformation on social media? In this research (N = 2,476), we show that the structure of online sharing built into social platforms is more important than individual deficits in critical reasoning and partisan bias—commonly cited drivers of misinformation. Due to the reward-based learning systems on social media, users form habits of sharing information that attracts others' attention. Once habits form, information sharing is automatically activated by cues on the platform without users considering response outcomes such as spreading misinformation. As a result of user habits, 30 to 40% of the false news shared in our research was due to the 15% most habitual news sharers. Suggesting that sharing of false news is part of a broader response pattern established by social media platforms, habitual users also shared information that challenged their own political beliefs. Finally, we show that sharing of false news is not an inevitable consequence of user habits: Social media sites could be restructured to build habits to share accurate information.
PBS Hacking Your Mind – Living on Autopilot – Episode 101 Aired: 09/09/20 According to Kahneman, when our slow-thinking system doesn’t have enough information to answer a question involving numbers, we simply stay on autopilot. And our autopilot system takes what might be called a shortcut and anchors its answer to the last number that crossed its radar, even when that number is completely irrelevant to the question at hand. -And that leads us to reach an absurd conclusion. I know it seems bizarre that anyone would do that, and surely you and I, reasonable people, would never do that in our real lives. Well, you do it all the time.
WebMD - Study: Antiviral Med Linked to COVID Mutations That Can Spread Written by Ralph Ellis Sept. 25, 2023 The study doesn’t say people should not use molnupiravir but calls for public health officials to scrutinize it. “The observation that molnupiravir treatment has left a visible trace in global sequencing databases, including onwards transmission of molnupiravir-derived sequences, will be an important consideration for assessing the effects and evolutionary safety of this drug,” the researchers concluded.
Democracy Now - Vaccine Inequity: Meet the Doctor Refusing a Booster as Rich Nations Get 16x More Doses Than Poor - October 28, 2021 Infectious disease expert Dr. Monica Gandhi says she will not receive a booster as a healthcare worker because of the global vaccine inequity, and argues the push for boosters “detracts from the fact that we in no way have fulfilled a moral and ethical obligation to the world.” We also speak with Kate Elder, senior vaccines adviser for Doctors Without Borders, who says that it is a structural issue caused by global leaders who are not “equitably sharing vaccines around the world.”
Anti-mask Woke-washing The moral distortion of social justice. CHLOE HUMBERT AUG 31, 2023 Michael Shellenberger has attempted to frame climate activists as doing “colonialism” and claim that reducing fossil fuel usage, to preserve the habitability of the planet for humans, is supposedly a human rights offense against people of the Global South.3 In a Climate Action Against Disinformation report titled ‘DENY, DECEIVE, DELAY’ this framing of “withholding fossil fuels” strangely overlaps with “anti-woke” narratives, and not surprisingly climate skepticism. In those PR spin zones they don’t mention how people in the Global South have already been harmed by the fossil fuel industry,4 and how people in the Global South are among the first harmed by climate change, such as in Bangladesh.5 People reportedly use similar upside down woke-washing arguments to defend tech projects such as Worldcoin, which Paris Marx reports has been deployed in the Global South luring people to “orbs” with tokens and free t-shirts, in order to collect biometric data from people and train the company’s computer systems.6 Molly White described “disingenuous arguments” on the Tech Won’t Save Us podcast, saying “I think that it's also used to silence a lot of the criticism against the projects here where you will speak out against something like Worldcoin or even crypto more broadly and people will say that’s just your white American privilege. You have financial privilege to dismiss these technologies. Can’t you see how these projects are helping people in developing countries? But what we've seen actually play out is broadly that they are NOT helping people. You know that the people who are engaging with these projects in those locations are suffering for it and often being exploited.”
MEDPageToday: Who's Really the Victim Here? — It's time to end DARVO behavior in the healthcare workplace by Resa E. Lewiss, MD, David G. Smith, PhD, Shikha Jain, MD, W. Brad Johnson, PhD, and Jennifer Freyd, PhD Perpetrators use DARVO because it works. In one study researchers found that targets of DARVO were more likely to blame themselves. Self-blame is associated with self-silencing. In another study, researchers found that observers of DARVO tended to doubt the credibility of the true victim, believing the perpetrator instead. There is not yet systematic data on what makes certain institutions and certain people more likely to DARVO. Yet, there appear to be relevant characteristics associated with other types of harassment, and the field of medicine checks all the boxes: high prestige, male-dominated institutions and industries, hierarchical leadership structures, inadequate safeguards for employees and trainees, and a climate which tolerates harassment.
Bizarre and Dangerous Utopian Ideology Has Quietly Taken Hold of Tech World “It's shaping our world right now,” says philosopher and historian Émile P. Torres. By Kelly Hayes,Truthout Published July 20, 2023 Here’s one example, Eliezer Yudkowsky, who more or less founded the rationalist community, and is a transhumanist singularitarian, who participated in the extropian movement. His views these days are very closely aligned to effective altruism and longtermism. He has a foot in just about all of these ideologies within the TESCREAL bundle. He has suggested that morality should be much more about number crunching than a lot of us would naturally suspect. For example, he published a blog post on a website called LessWrong, which he founded in 2009. That’s sort of the online epicenter of the rationalist community. In this blog post, he asked a question, what would be worse: one individual being tortured mercilessly for 50 years straight? Just endless interminable suffering for this one individual, or some extremely large number of individuals who have the almost imperceptible discomfort of having an eyelash in their eye? Which of these would be worse? Well, if you crunch the numbers, and if the number of individuals who experience this eyelash in their eye is large enough, then you should choose to have the individual being tortured for 50 years, rather than this huge number of individuals being slightly bothered by just a very small amount of discomfort in their eye. It’s just a numbers game. And so he refers to this as the heuristic of shut up and multiply.
BBC - Anthony Fauci on the recent spike in Covid cases - 28th August 2023, 08:18 ED Doctor Anthony Fauci: “You’ll find the vulnerable will fall by the wayside. They’ll get infected, they’ll get hospitalized and some will die.
CDC made medical guidelines please Delta Airlines, and now lots of people work sick and contagious in every industry Chloe Humbert Jan 10, 2024 Delta Airlines sent a letter to the CDC on December 21, 2021 complaining that the 10 day isolation guidelines were interfering with their operations because of people being off sick too often. Instead of better infection control, stopping the spread among staff, or hiring more staff to cover the “new normal” of everyone getting covid on the job all the time, they instead asked the CDC to reduce the isolation time recommended. On December 27, 2021, the CDC complied with Delta Airlines request and reduced the guideline for isolation down to 5 days. This is the supposedly scientifically guided medical advice for isolation time, for public health and the wellbeing of citizens. But instead they sided with the corporations.
The Pfizer earnings call: profits driven by surges. Another case of privatized profits & socialized losses with too many coincidences. CHLOE HUMBERT OCT 2, 2022 Angela Hwang - Pfizer Inc. - Group President of Biopharmaceuticals Group: “So I think when you add all of this up, what we are seeing is the fact that there is demand for this product. We also see that the social -- the removal of the mask mandate, the social distancing requirements that have been removed. You also know that in the EU that just in the last week, they've removed the emergency period of the EUA. That means that people are going to get out there. We know with all of that, infections are going to increase, and that's the role that PAXLOVID can play.”
Walker Bragman: Pfizer Spends Big on IP Lobbying With Billions On the Line. The pharmaceutical giant spent big bucks amid key international negotiations last year to protect record earnings. - Important Context MAR 9, 2023 The pharmaceutical industry and Pfizer, in particular, have fought hard to prevent any proposed waivers of IP protections. According to an October 2022 report from The Bureau of Investigation Journalism, days after the Biden administration announced its support for an IP waiver for vaccines, Pfizer met with UK trade policy minister Greg Hands, vaccines minister Nadhim Zahawi, and international trade secretary Liz Truss.
Drugwatch - Zithromax (azithromycin), also known as Z-Pak Zithromax has been highly profitable for its manufacturer, Pfizer. At the height of sales in 2002, it brought in over $1 billion for Pfizer. Although the wide availability of generics reduced the company’s revenue, sales still totaled $435 million in 2012.
Ajufo E, Rao S, Navar AM, Pandey A, Ayers CR, Khera A. U.S. population at increased risk of severe illness from COVID-19. Am J Prev Cardiol. 2021 Jun;6:100156. doi: 10.1016/j.ajpc.2021.100156. Epub 2021 Feb 13. Erratum in: Am J Prev Cardiol. 2021 Jun;6:100195. PMID: 33615285; PMCID: PMC7880833. Results: An estimated 176.1 million individuals representing 75.4% of U.S. adults had at least one increased-risk condition, 40.3% ≥2 and, 18.5% ≥3 conditions. Approximately 129 million adults aged <65 (69.2%) were also estimated to be at increased-risk. Compared to Whites, similar proportions of Blacks in the overall population (78.0 vs. 75.6%, p>0.05) and Hispanics in the younger population (70.8 vs 68.4%) were estimated to be at increased-risk. Conversely, a greater proportion of individuals with lower education and income levels were estimated to be at increased-risk both in the overall and younger population. In addition, an estimated 6.2 million individuals (14.5%) had heart disease. Among these, virtually all had at least one additional CDC risk factor (97.9%) and most had ≥2 or ≥3 risk factors (83.8% and 58.5%, respectively). Conclusions: As vaccination strategies are being explored, these results demonstrate that >75% of adults in the U.S. would be considered at increased-risk for severe COVID-19 infection by CDC criteria. Risk factor prevalence alone may not adequately capture the totality of risk, particularly among Black and Hispanic racial/ethnic groups and those with heart disease.
Hail Mary, noun - dictionary.com Also called Hail Mary pass, Hail Mary play . a long forward pass in football, especially as a last-ditch attempt at the end of a game, where completion is considered unlikely.
ESSENTIAL SERVICES NEED MASK REQUIREMENTS A letter to send to government representatives, healthcare providers, transit authorities, store managers, and community leaders. (2.0) CHLOE HUMBERT APR 12, 2023 Mask requirements are necessary at essential services to keep these services accessible by mitigating the hazard. One-way masking is not even possible at the DMV, dentists, and healthcare settings where people need to remove masks. Public transit, medical waiting rooms, and government offices are often poorly ventilated crowded areas which are known to promote the spread of disease. Source control is vital. High risk people need to access services.
Image slide from a presentation by Ruth Link-Gelles, at the CDC Advisory Committee on Immunization Practices (ACIP) meeting in September 2022, a graph showing vaccine effectiveness (VE) against symptomatic infection, waning for all age groups to around zero by 8 months, with profound waning at 6 months. Image source is a CDC program, Increasing Community Access to Testing (ICATT): VE analysis for symptomatic infection.
Multiple layers for safety: public health is not an à la carte menu. Successful safety interventions are about a comprehensive commitment to the common good. CHLOE HUMBERT OCT 15, 2023 The Swiss Cheese Model of public health pandemic mitigations is supposed to demonstrate the need to use all safe & effective tools available because none are guaranteed perfect, all have weaknesses, so you use them all together to reap the benefits of the barrier created by the collective implementation
Federal Trade Commission (FTC) - Disclosures 101 for Social Media Influencers The FTC works to stop deceptive ads, and its Endorsement Guides go into detail about how advertisers and endorsers can stay on the right side of the law. If you endorse a product through social media, your endorsement message should make it obvious when you have a relationship (“material connection”) with the brand.
U.S. SECURITIES AND EXCHANGE COMMISSION - Press Release SEC Charges Kim Kardashian for Unlawfully Touting Crypto Security FOR IMMEDIATE RELEASE 2022-183 Washington D.C., Oct. 3, 2022 — The Securities and Exchange Commission today announced charges against Kim Kardashian for touting on social media a crypto asset security offered and sold by EthereumMax without disclosing the payment she received for the promotion. Kardashian agreed to settle the charges, pay $1.26 million in penalties, disgorgement, and interest, and cooperate with the Commission’s ongoing investigation. The SEC’s order finds that Kardashian failed to disclose that she was paid $250,000 to publish a post on her Instagram account about EMAX tokens, the crypto asset security being offered by EthereumMax. Kardashian’s post contained a link to the EthereumMax website, which provided instructions for potential investors to purchase EMAX tokens. "This case is a reminder that, when celebrities or influencers endorse investment opportunities, including crypto asset securities, it doesn’t mean that those investment products are right for all investors," said SEC Chair Gary Gensler. "We encourage investors to consider an investment’s potential risks and opportunities in light of their own financial goals."